

What is the structure and function of the urinary bladder?
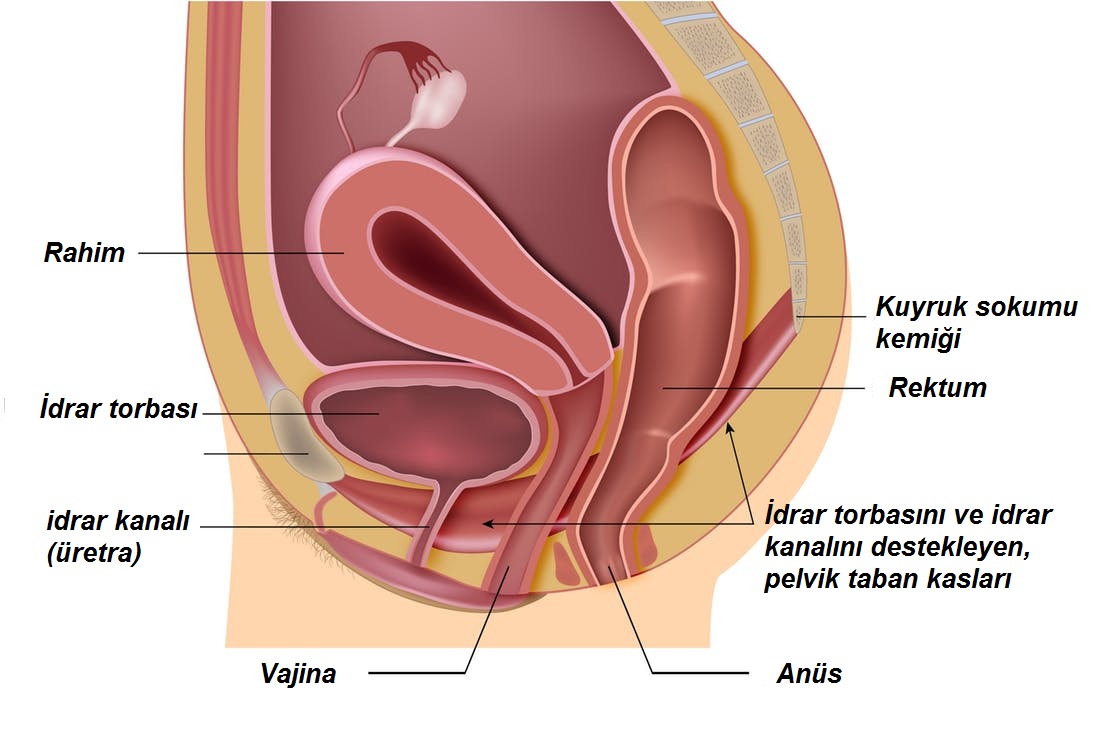
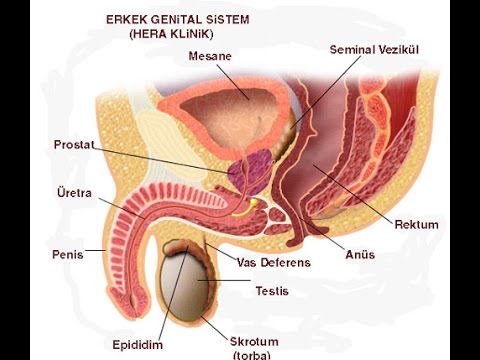
The urinary bladder (Bladder) is where the urine produced in the kidneys accumulates. There is a canal called the ureter between the bladder and kidneys. There is a canal (urethra) that runs under the bladder and arises from the penis in men and just above the vagina in women. In men, the urinary bladder is situated in front of the intestines, while in women, it is located under the uterus. This organ resembles a hollow orange-sized ball of muscles, but it has an elastic structure that shrinks when empty and expands when filled. Between 350 and 500 mL of urine can accumulate in the bladder of a normal individual.
What is bladder cancer?
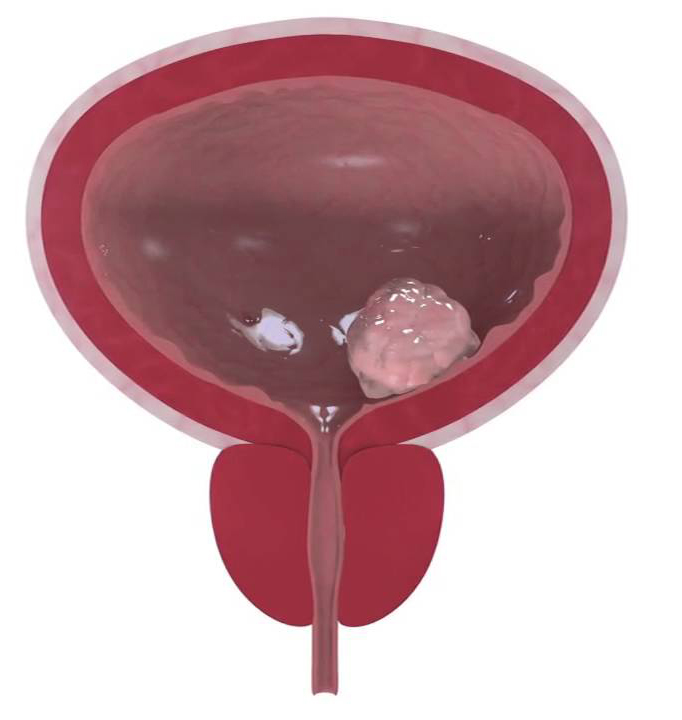
The bladder may have many diseases such as inflammation (cystitis), benign tumors, excessive activity, dysfunction, shrinkage, or cancer development. Bladder cancer, like other forms of cancer in the body, is caused by abnormal cell growth in the bladder. The inner layer of the urinary bladder has a different structure, with a muscle layer underneath it that helps it to contract and retain its elastic structure. The bladder is covered and protected by a membrane on its outer surface. Many different tissues, such as blood vessels, nerves, and fat cells, make up this structure. Each of these systems has the potential to grow cancer. Cancer is named for the structure from which it emerges, but the most common form arises from the cells that line the inner surface. It is called Transitional Cell Carcionam (TCC) and it accounts for more than 90% of all bladder cancers. This tumor usually has the appearance of a cauliflower developing in the bladder with a smooth inner surface.

What causes bladder cancer?
Smoking is the most obvious aspect that can be mentioned in this context. Apart from this, exposure to chemicals used in some factories is also thought to cause bladder cancer.

What are the symptoms of bladder cancer?
The most obvious complaint of bladder cancer IS BLOODY URINE WITHOUT PAIN AND BURNING. Aside from that, it may also cause problems such as urination trouble and repeated urination. Patients with visible bleeding in the urine should consult a urologist immediately. However, it should be remembered that bladder cancer is not the only source of urinary bleeding. Therefore, the doctor should be the one to make this distinction.
5- What are the methods of bladder cancer diagnosis?
The first step in making a diagnosis is taking a comprehensive medical history and doing a thorough physical examination on the patient. After this point, urinalysis and ultrasonography, in particular, are typically enough to make the first diagnosis. Ultrasonography can detect tumors in the urinary bladder if they are not too small. The second stage is to test the urinary bladder with endoscopic instruments with cameras in patients who have bleeding in the urine but no findings on ultrasound (cystoscopy). The mass discovered during cystoscopy is extracted, and the cause of the mass is determined and treated.
Cystoscopy: This operation can be performed under general, spinal (narcotization from the waist), or local anesthesia (narcotizing only the urinary canal). A camera device is used to gain access to the bladder via the urinary hole. The entire bladder is inspected in-depth, and if a mass is found, it is scraped and removed. The extracted part must then be examined by the pathology.
The final diagnosis is made according to the pathology result. The pathology report shows the cancer type, aggressiveness, and whether cancer has spread to the bladder’s depths. This information determines the patient’s treatment process.

What Are Bladder Cancer Treatment Methods?
As mentioned earlier, there are several types of bladder cancer and the most common type is TCC. This type, on the other hand, has a variety of forms with varying degrees of aggression. Apart from this, some types of this cancer are only in the inner surface of the bladder, while others spread deeper. In addition to these, many other factors are taken into consideration when evaluating treatment options;
- – The type of cancer
- – How deep is the cancer?(superficial, deep)
- – Stage of cancer (spread status)
- – Cancer grade (aggressiveness status)
- – Size of cancer (diameter)
- – The amount of cancer (there may be more than one tumor in the bladder)
- – Whether it has recurred
- – Presence of metastasis etc.
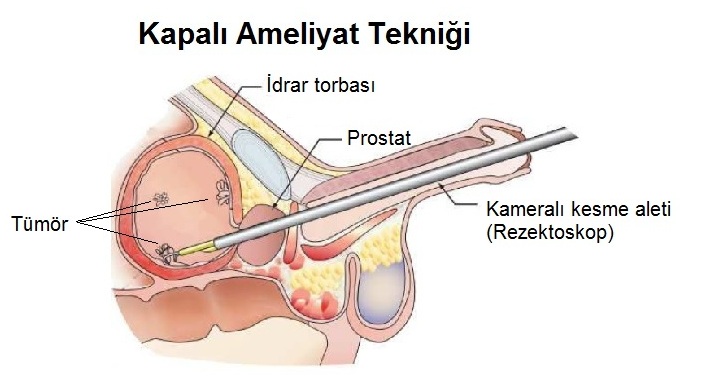
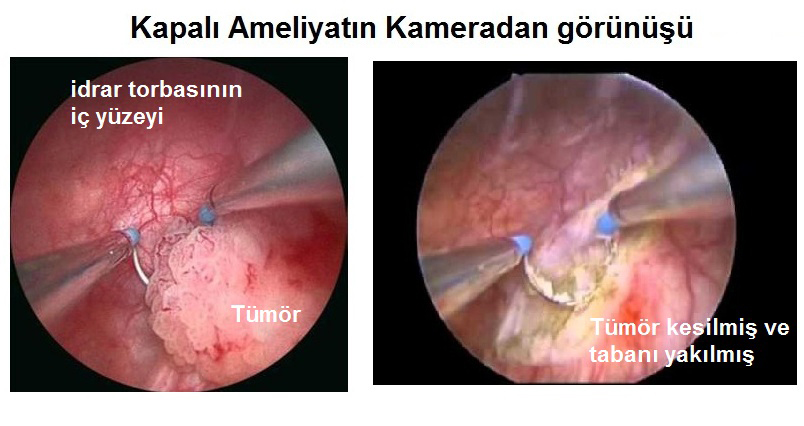
Cystoscopy and TUR-M: Cystoscopy is the first technique used in patients who have been diagnosed with bladder cancer using films such as ultrasonography or tomography. As previously reported, this technique is useful for diagnosis, and the patient is treated if the cancer can be absolutely scraped from here. However, in some cases, this technique is sufficient for treatment, but in others, it can be just the first step of the treatment process. This is the process of treating bladder cancer with a closed method and is called (TUR-M).
After this stage, the patient’s follow-up and treatment protocols are determined based on the result from the pathology. Either of the following outcomes can occur as a result of the pathology, and the treatment and follow-up scheme will be adjusted accordingly.
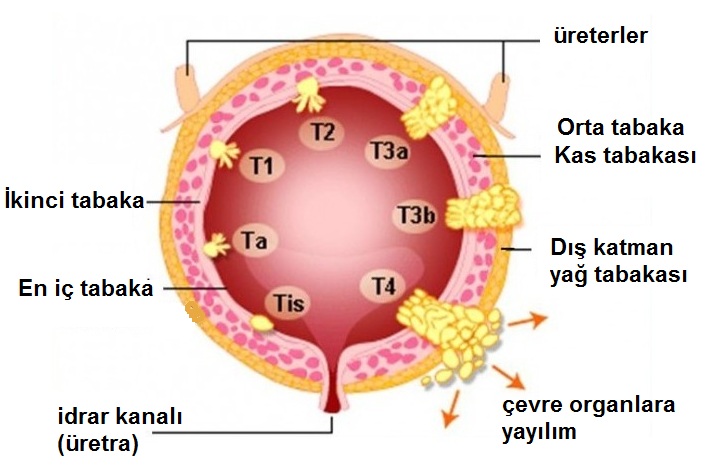
) CIS: This result indicates that the tumor is very superficial but may progress aggressively. Other tumors are often located in the vicinity of the primary tumor. Patients are taken to 3-month cystoscopy follow-up. Depending on the patient’s condition, a procedure in which medicine is injected into the bladder via a catheter may be initiated.
b) Ta: This indicates that the tumor is located in the first layer of the bladder’s inner surface. These patients normally do not need further treatment, but cystoscopy must be repeated after 3 to 9 months. Following that, the patient is followed up with cystoscopy at regular intervals.
c) T1: It shows that the tumor occupies the layer below the inner surface (the second layer) of the bladder. These patients should be followed up more closely and should receive additional treatment. The first step is to repeat the cystoscopy approximately 4-6 weeks later. In this procedure, by scraping again from the old scraping area, it can be determined if the tumor is deeper or not. If the result is again T1, drug therapy is started at this stage. There are two types of medications that can be used here, but none are oral or intravenous. These medications are administered to the patient by inserting a catheter into the urine bag.
After the drug is administered, the catheter is removed and the patient is asked not to go to the toilet for 2 hours. Depending on the patient’s condition, the medication is given for 1 or 3 years, once a week for 6 weeks, then once a month. Meanwhile, the cystoscopy procedure should be repeated every 3 months. If the tumor develops again in the intervening cystoscopy, then the treatment may change.
d) T2: Indicates that the tumor has reached the middle layer, the muscle layer. For these patients, surgery to remove the whole urinary bladder is the only option. This surgery is called Radical Cystectomy. After the urinary bladder is removed, a new urinary bladder is made from the patient’s own intestine This bladder is either attached to the skin on the side of the patient’s abdomen or attached to his own urinary canal.
e) T3: Indicates that the tumor has reached the outer membrane of the urinary bladder. In this case, a thorough examination is needed to determine if cancer has spread to other organs. These patients will also undergo Radical Cystectomy surgery if cancer has not spread, but they would most likely need chemotherapy after the operation.
f) T4: Indicates that the tumor has spread to organs adjacent to the urinary bladder. Films (radiology), not pathology, are commonly used to make this diagnosis. Chemotherapy and Radiotherapy should be applied to these patients.